Skip to content
About
Expand
About ISAPP
Board of Directors
Topics
Expand
Probiotics
Prebiotics
Synbiotics
Postbiotics
Fermented Foods
Live Dietary Microbes
Gut Health
Microbiome
All Topics
Resources
Expand
Videos
Publications
Podcasts
Infographics
All Resources
News/Blog
Get Involved
Expand
Scientists
Clinicians
Industry
Media & Science Communicators
Consumers
Students
Donate
Awards
Events
Search for:
Search
Account
Member Login
Contact
Account
Search
Search
Toggle Menu
bifidobacterium
1-1 of 1 results
Sort by
Sort by title (Z-A)
Sort by title (A-Z)
Sort by newest
Sort by oldest
News/Blog
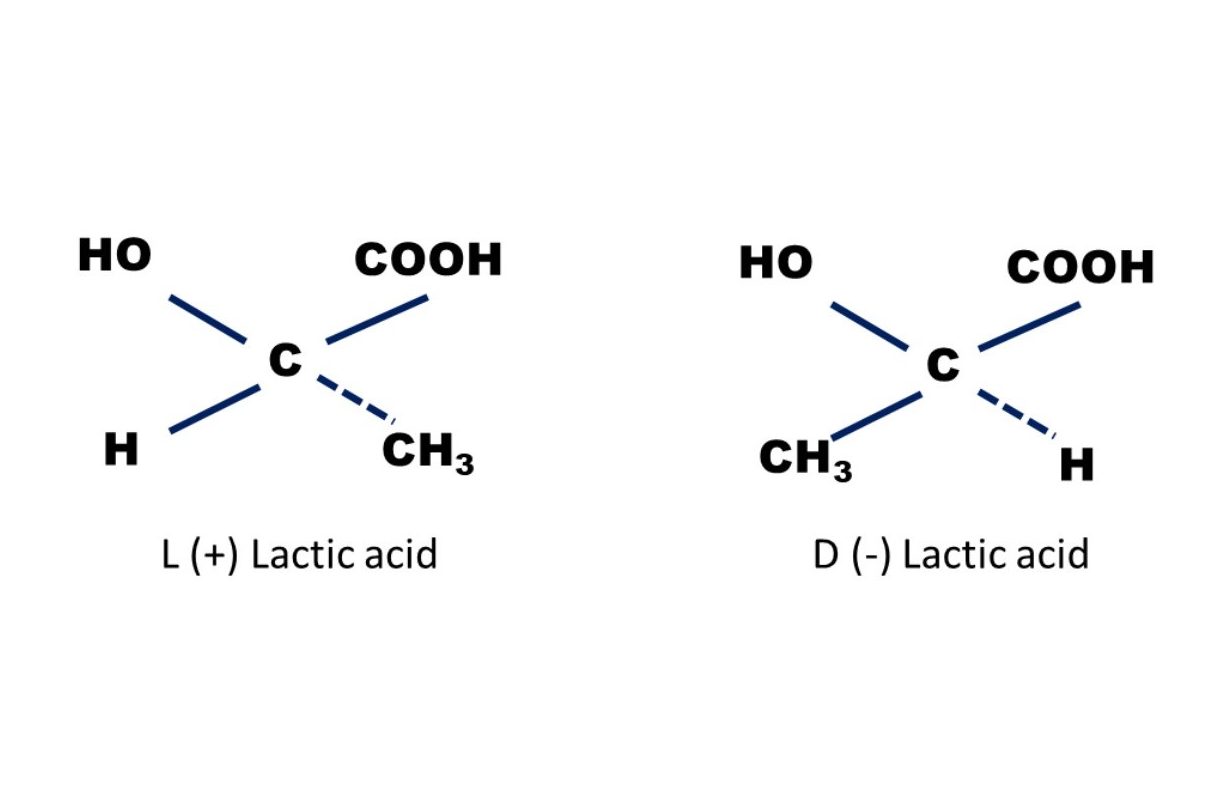
‘Brain fogginess’ and D-lactic acidosis: probiotics are not the cause
Mary Ellen Sanders PhD, Executive Science Officer, International Scientific Association for Probiotics and Prebiotics Bruno Pot PhD, Research Group of…
Scroll to top
Scroll to top
About
Toggle child menu
Expand
About ISAPP
Board of Directors
Topics
Toggle child menu
Expand
Probiotics
Prebiotics
Synbiotics
Postbiotics
Fermented Foods
Live Dietary Microbes
Gut Health
Microbiome
All Topics
Resources
Toggle child menu
Expand
Videos
Publications
Podcasts
Infographics
All Resources
News/Blog
Get Involved
Toggle child menu
Expand
Scientists
Clinicians
Industry
Media & Science Communicators
Consumers
Students
Donate
Awards
Events
Toggle Menu Close
Search for:
Search