1-12 of 12 results
-

Probiotics with antibiotics: Let’s follow the evidence
In this blog, experts address a media article on probiotics with antibiotics and advocate for using evidence instead of weak but plausible-sounding recommendations. -

Emerging clinical insights into C. difficile infection from gut microbiota research
In recent years the clinical status and spectrum of C. difficile infection have shifted. The prevalence of this infection has risen sharply. Along with changes that have occurred in the clinical patterns of this disorder, research on the gut microbiome has provided insights into the important factors that contribute to the infection. -

Probiotics vs. prebiotics: Which to choose? And when?
As consumers, we are constantly bombarded with information on what we should eat to improve our health. Yet the information… -

Do antibiotics ‘wipe out’ your gut bacteria?
By Dr. Karen Scott, University of Aberdeen, UK Antibiotics have been an important tool in medicine to kill pathogenic bacteria… -

Probiotics: Money Well-Spent For Some Indications
Eamonn M M Quigley MD, Houston Methodist Hospital and Weill Cornell Medical College, Houston, Texas, USA; Hania Szajewska MD, The… -

Late initiation of probiotic therapy for acute pediatric gastroenteritis may account for null results
Francisco Guarner, MD, PhD, University Hospital Vall d’Hebron, Barcelona, Spain; Michael Cabana, MD, MPH, University of California, San Francisco, CA,… -

ISAPP-initiated systematic review and meta-analysis shows the association of probiotic consumption with reduced antibiotic prescriptions
At the ISAPP meeting in Turku, Finland in 2016, scientists convened a working group led by Dan Merenstein of Georgetown… -

Clinical evidence and not microbiota outcomes drive value of probiotics
By ISAPP Board of Directors, plus Prof. Francisco Guarner and Dr. Bruno Pot September 10, 2018 Two recent papers have… -
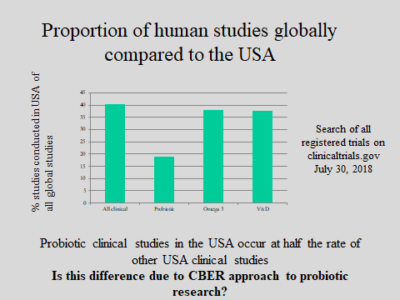
CBER to hold public workshop on regulation of biologics
FDA’s Center for Biologics Evaluation and Research (CBER) is convening a public workshop Sept 17 in Rockville MD on the… -

ISAPP Goes to India
By Mary Ellen Sanders PhD and Dan Merenstein MD ISAPP sent two key-note speakers to the Probiotics Association of India… -
ISAPP works to have evidence-based usage of probiotics to prevent antibiotic-associated diarrheoa implemented in UK
January 12, 2018. Antibiotics are amongst the most commonly prescribed drugs in UK hospitals. However, as well as treating infection… -
The Times They Are A-Changin’ With Probiotics
I had a surprising encounter a few weeks ago in the clinic. I was caught off guard, had to take…

